Introduction
Learning how to write SOAP notes effectively is essential for healthcare professionals. This structured documentation format helps clinicians record patient encounters with clarity and precision. If you’re wondering how to write SOAP notes properly, this comprehensive guide will walk you through the process step by step, providing practical examples and best practices.
This guide explores everything healthcare professionals need to know about crafting effective SOAP notes, from understanding their core structure to implementing them efficiently within your practice management system.
How to Write SOAP Notes: Understanding the Basics
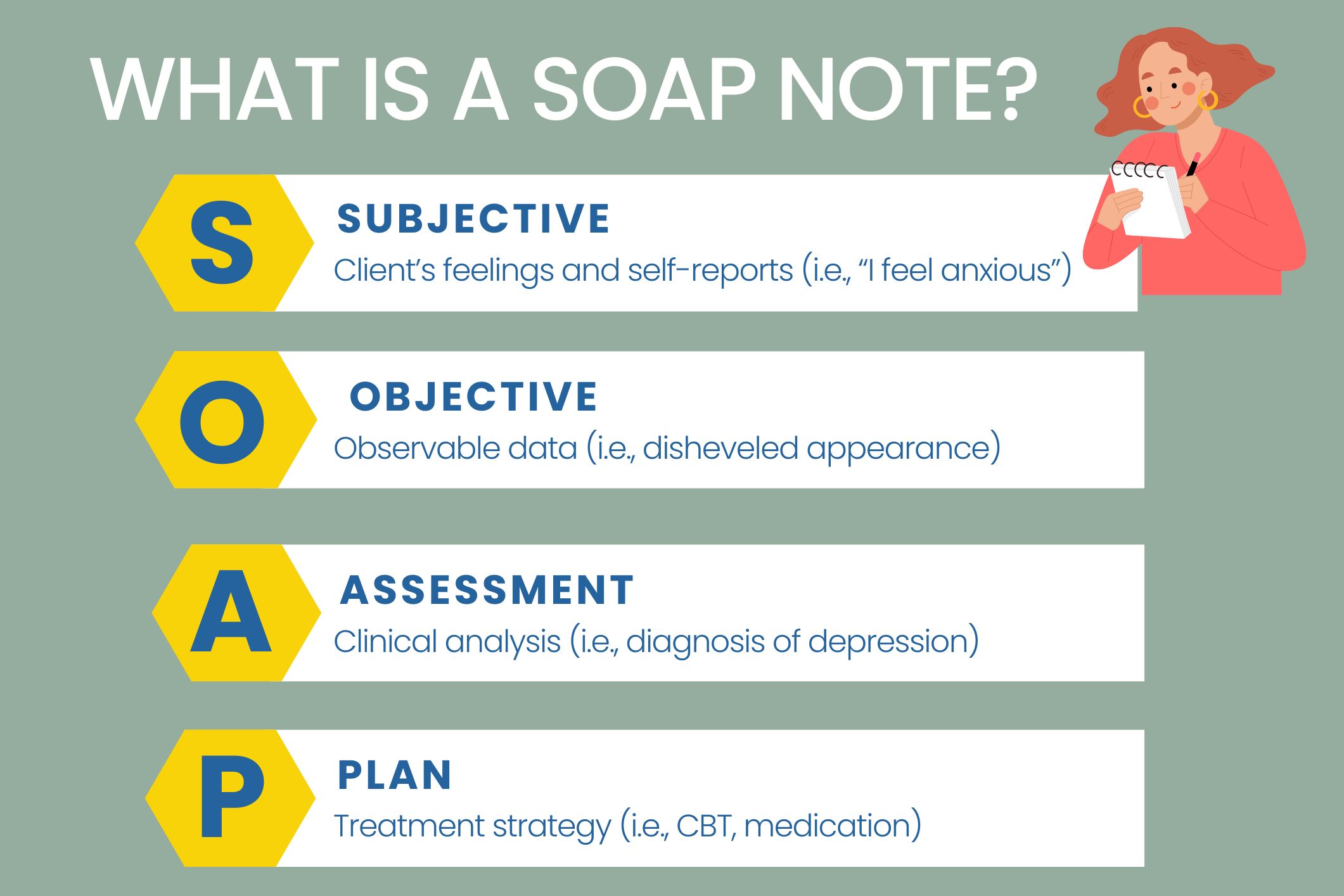
SOAP notes are a standardised documentation format used by healthcare providers to record patient encounters. Learning how to write SOAP notes effectively begins with understanding what the acronym SOAP stands for:
- Subjective: Patient’s reported symptoms and experiences
- Objective: Observable clinical findings
- Assessment: Clinical analysis and diagnosis
- Plan: Treatment strategy and next steps
Developed in the 1950s by Lawrence Weed, a professor at Yale University, this method was initially known as a problem-oriented medical record (POMR). Today, SOAP notes serve as a universal framework across healthcare disciplines, from medicine and nursing to mental health services and allied health professions.
The beauty of SOAP notes lies in their clarity and consistency. With a structured approach to documentation, providers can:
- Track patient progress systematically
- Share information effectively with other healthcare professionals
- Create legally sound medical records
- Support clinical decision-making with organised data
How to Write SOAP Notes: The Four Essential Components
Let’s examine each section of the SOAP format in detail to understand what information belongs where when learning how to write SOAP notes effectively.
1. Subjective Section
The Subjective section captures the patient’s perspective—what they tell you about their condition, symptoms, concerns, and experiences. This section relies primarily on patient-reported information rather than clinical observations.
What to include:
- Chief complaint or presenting problem
- Symptom descriptions (onset, duration, severity, aggravating/alleviating factors)
- Patient’s medical and mental health history
- Current medications
- Information provided by family members
- Relevant social history
Example entry: “Patient reports increased anxiety over the past week, describing feelings of restlessness and difficulty concentrating. States that symptoms worsen during work meetings and when attempting to sleep. Reports no change in medication regimen.”
Important tip: Always attribute statements in this section to their source—whether the patient, family member, or previous medical record—to distinguish reported information from clinical fact.
2. Objective Section
The Objective section contains factual, observable data collected during the clinical encounter. This includes your direct observations, examination findings, test results, and measurable information.
What to include:
- Vital signs
- Physical examination findings
- Mental status observations
- Results from assessments or screening tools
- Laboratory or diagnostic test results
- Patient’s appearance, behaviour, and demeanour during the session
Example entry: “Patient appeared tense with visible hand tremors. Speech was rapid with frequent topic changes. Blood pressure measured at 138/88. Scored 14 on GAD-7 anxiety screening (moderate-severe range). Maintained minimal eye contact throughout session.”
Important tip: Keep this section strictly factual and based on your direct observations—not the patient’s reports or your interpretations.
3. Assessment Section
The Assessment section represents your clinical analysis of the information gathered. Here, you synthesise the subjective and objective data to formulate a diagnosis or clinical impression.
What to include:
- Current diagnosis or list of potential diagnoses
- Clinical reasoning behind your assessment
- Reference to diagnostic criteria (e.g., DSM-5)
- Changes in condition compared to previous sessions
- Risk assessment information
- Progress toward treatment goals
Example entry: “Based on reported symptoms and clinical observations, patient continues to meet criteria for Generalised Anxiety Disorder (F41.1). Anxiety symptoms have intensified compared to previous session, likely related to upcoming work presentation. No evidence of suicidal ideation or intent.”
Important tip: Your assessment should logically follow from the information presented in the subjective and objective sections.
4. Plan Section
The Plan section outlines your strategy for addressing the issues identified in your assessment. This includes immediate interventions, referrals, and long-term treatment planning.
What to include:
- Treatment interventions for current session
- Homework or between-session activities
- Medication recommendations or changes
- Referrals to other providers
- Follow-up appointment schedule
- Specific goals for future sessions
- Expected outcomes and timeline
Example entry: “Will continue cognitive-behavioural therapy focusing on thought challenging techniques. Recommended daily mindfulness practice using provided audio recordings. Referred to GP for evaluation of possible medication management. Scheduled weekly sessions for next month to monitor progress.”
Important tip: Be specific about action items, responsibilities, and timelines to create a clear roadmap for treatment.
How to Write SOAP Notes for Different Specialities: Examples
Different healthcare disciplines may emphasise certain sections of SOAP notes based on their specific focus. Here are examples showing how to write SOAP notes for two different specialities:
Mental Health Therapy SOAP Note Example
Subjective: Patient reports feeling more anxious this week. She described feeling “jittery and on-edge” with increased difficulty controlling worried thoughts. States she’s been sleeping poorly, averaging 5 hours per night compared to her usual 7 hours.
Objective: During the session, patient displayed visible restlessness, repeatedly wringing hands and shifting position. Speech pattern was rapid with frequent pauses to recollect thoughts. Patient asked for questions to be repeated several times. Expressed fears about job security and housing stability despite acknowledging no concrete evidence these were at risk.
Assessment: Patient’s anxiety symptoms have intensified but remain consistent with previously diagnosed Generalised Anxiety Disorder (F41.1). Current stressors include upcoming work performance review and financial concerns. No indications of comorbid depression or substance use issues.
Plan: Recommended patient consult with GP to rule out thyroid dysfunction or other physiological contributors to anxiety. Will continue weekly therapy sessions using cognitive-behavioural approach. Introduced progressive muscle relaxation technique in session and provided recorded guide for daily practice at home. Will focus next session on identifying and challenging catastrophic thinking patterns.
Speech-Language Pathology SOAP Note Example
Subjective: Patient reports increased vocal demands since previous session due to additional work meetings. Notes colleagues positively commented that her “voice is back” after recent presentation. Still experiences intermittent vocal fatigue during extended social interactions. Reports consistent adherence to recommended semi-occluded vocal tract straw (SOVT) exercises three times daily for five minutes.
Objective: Led patient through SOVT exercises with straw in water. Patient independently achieved optimal voicing in 5/5 opportunities with appropriate back pressure. During conversational training therapy (CTT), patient successfully differentiated between “husky” voice and “presenter” voice in 5/5 prompted trials. When practising functional phrases, patient achieved target “presenter” voice in 8/10 opportunities with moderate visual cueing. Patient self-rated vocal effort during CTT exercises as 4/10 (mild).
Assessment: Patient demonstrates significant improvement in vocal production techniques to meet professional speaking demands, as evidenced by reduction in self-rated vocal effort from 7/10 to 4/10. Successfully integrating learned strategies into workplace communication. Continued practice needed for carryover to social communication contexts where fatigue remains a factor.
Plan: Continue current treatment approach with focus on generalising vocal techniques to social settings. Introduce additional compensatory strategies for managing vocal load throughout the day. Recommended voice amplification tool for use during extended speaking engagements. Scheduled biweekly sessions for next month to monitor progress and adjust home programme as needed.
How to Write SOAP Notes Effectively: Best Practices
To maximise the effectiveness of your SOAP documentation and learn how to write SOAP notes that truly serve their purpose, consider these practical recommendations:
Be Concise Yet Comprehensive
Strike a balance between brevity and thoroughness. Include all relevant clinical information without unnecessary detail or repetition. Focus on information that directly impacts diagnosis and treatment planning.
Use Objective Language
Maintain professional, non-judgmental language throughout your documentation. Avoid subjective interpretations in the Objective section, and clearly differentiate between patient reports and clinical observations.
Stay Organised
Follow the SOAP structure consistently. Keep information in its appropriate section to maintain clarity and prevent confusion when others review your notes.
Document in Real-Time When Possible
Complete your notes as soon as possible after patient encounters while details remain fresh. Delayed documentation increases the risk of forgotten information and inaccuracies.
Focus on Clinical Relevance
Include information that’s pertinent to the patient’s current condition and treatment. Avoid irrelevant details that don’t contribute to clinical understanding or care planning.
Use Specific Measurements
Whenever possible, quantify your observations with specific measurements rather than vague descriptors. For example, “scored 14 on GAD-7” is more informative than “showed moderate anxiety.”
Document Changes and Progress
Highlight changes in the patient’s condition compared to previous sessions. This helps track progress and justify continued treatment.
Consider Legal and Ethical Requirements
Remember that clinical notes are legal documents. Maintain confidentiality, document informed consent discussions, and include risk assessments when appropriate.
Implementing SOAP Notes in Your Practice
Integrating SOAP notes into your clinical workflow can significantly enhance your documentation efficiency. Here are some implementation strategies:
Use Digital Templates
Many electronic health record (EHR) systems offer customisable SOAP note templates. These templates can streamline documentation by providing structured fields for each SOAP component.
Develop Specialty-Specific Templates
Create or adapt templates that address the specific documentation needs of your clinical specialty, including relevant assessment tools and intervention options.
Establish Documentation Routines
Set aside dedicated time for documentation immediately following patient appointments. Consistency in your documentation schedule prevents backlogs and improves accuracy.
Train Support Staff
If applicable, train administrative or clinical support staff to assist with certain aspects of documentation, such as entering objective data or updating plan components like appointment scheduling.
Regularly Review Documentation Quality
Periodically audit your SOAP notes for completeness, clarity, and compliance with professional standards. This practice helps identify areas for improvement in your documentation approach.
Using SOAP Notes with Practice Management Systems
Modern healthcare practice relies increasingly on digital solutions for clinical documentation. Practice management systems streamline the SOAP note process through:
- Built-in templates that follow the SOAP structure
- Auto-population of patient demographics and clinical history
- Secure storage with appropriate access controls
- Integration with billing and scheduling functions
- Note cloning features that allow updating previous notes efficiently
When selecting a practice management system, look for one that offers customisable SOAP templates tailored to your specialty, secure cloud storage, and intuitive interfaces that minimise documentation time.
Common SOAP Note Pitfalls to Avoid
Even experienced clinicians can make documentation errors. Here are common mistakes to watch for:
- Mixing subjective and objective information: Keep patient reports in the Subjective section and your observations in the Objective section.
- Vague or incomplete assessment: Ensure your assessment clearly connects to the information presented and includes specific diagnoses when appropriate.
- Non-specific treatment plans: Avoid general statements like “continue therapy” without specifying interventions, frequency, or goals.
- Excessive copying from previous notes: While referencing prior information is helpful, excessive copying can perpetuate outdated information.
- Inappropriate abbreviations: Use only widely accepted medical abbreviations to prevent misinterpretation.
- Missing signatures or dates: Always include your electronic signature, credentials, and date/time documentation was completed.
When to Use SOAP Notes vs. Other Documentation Formats
While SOAP notes offer tremendous versatility, they may not be the optimal format for every clinical situation. Consider these alternatives for specific documentation needs:
- Progress notes: For brief updates between comprehensive evaluations
- BIRP notes: (Behaviour, Intervention, Response, Plan) Often used in behavioural health settings
- DAP notes: (Data, Assessment, Plan) A simplified alternative to SOAP
- Narrative notes: For complex psychosocial assessments requiring detailed history
Select the documentation format that best serves your clinical context while meeting legal and professional requirements.
Conclusion
Mastering SOAP notes represents an essential skill for healthcare professionals across disciplines. These structured documents facilitate systematic thinking, clear communication with colleagues, and comprehensive patient records that support quality care.
By following the guidelines outlined in this article, you can create SOAP notes that efficiently capture patient encounters while meeting professional and legal documentation standards. Whether you’re documenting therapy sessions, medical consultations, or rehabilitation visits, the SOAP format provides a consistent framework for clinical reasoning and treatment planning.
Key Takeaways: How to Write SOAP Notes Effectively
- Effective SOAP notes follow a four-part structure: Subjective, Objective, Assessment, and Plan
- When writing SOAP notes, maintain clear boundaries between subjective reports and objective observations
- Learn to be specific and concise while including all clinically relevant information
- To write effective SOAP notes, document in real-time whenever possible to maximise accuracy
- Utilise digital templates and practice management systems to streamline your SOAP note documentation
- Review your notes regularly for quality improvement
- Remember that effectively written SOAP notes serve multiple purposes: communication, clinical reasoning, legal documentation, and continuity of care
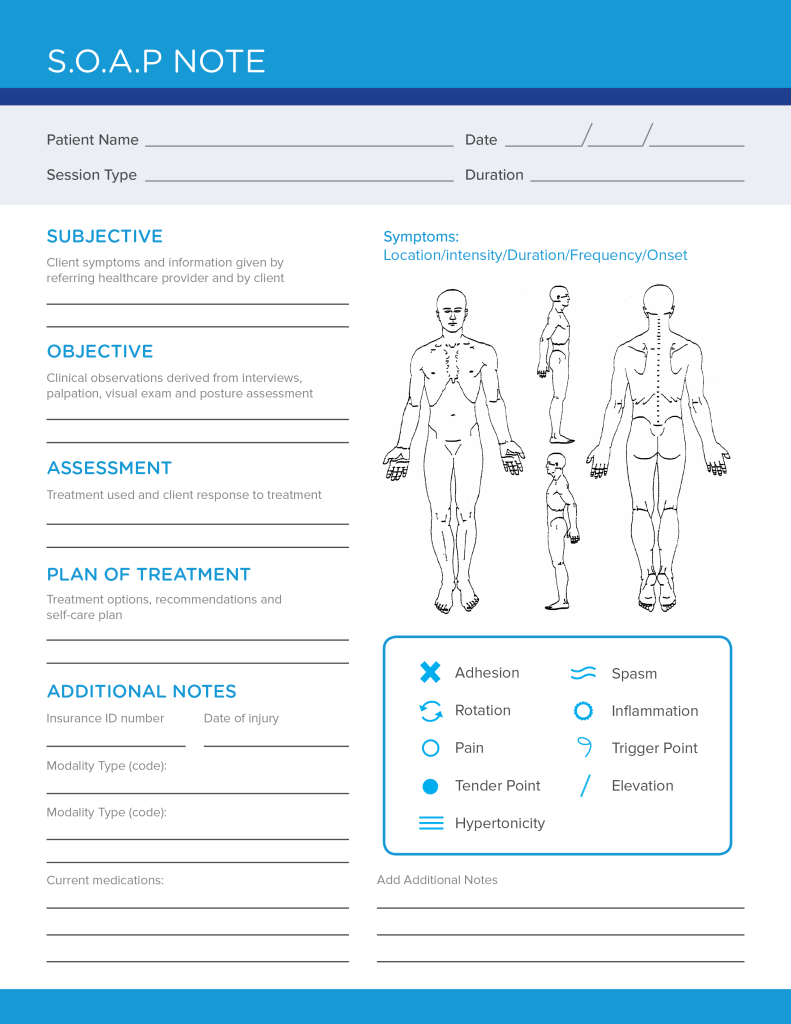
Download our free SOAP note template to get started with structured clinical documentation today.